Fetal circulation Shunts Chemical substances alterting the flow Flow dynamics Oxygenation Changes at birth Remnants of the fetal circulation components.
STUDY NOTES:
FETAL CIRCULATION & SHUNTS
DIFFERENCE OF FETAL CIRCULATION FROM AN ADULT CIRUCLATION
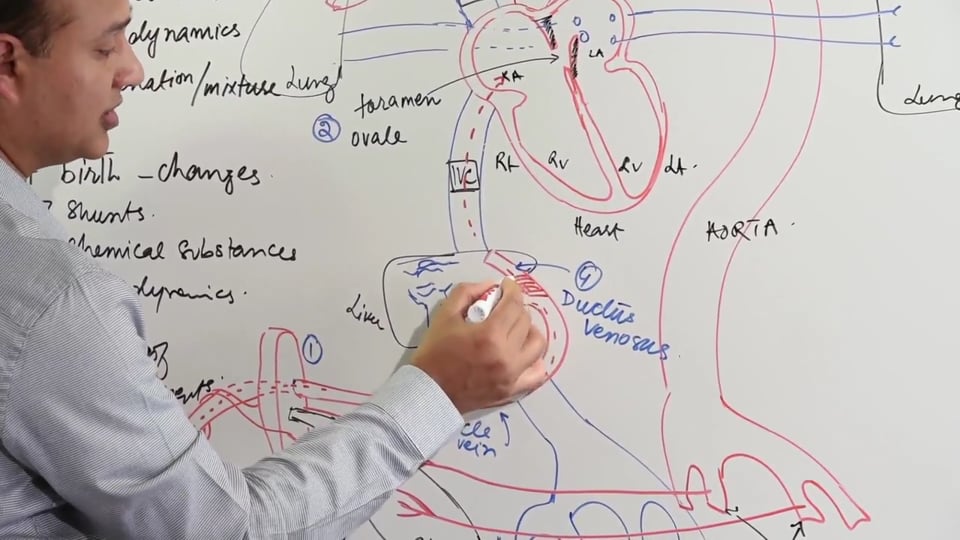
• The fetus has a connection with the maternal blood supply at the site of placenta. This connection is formed by the two umbilical arteries and a single umbilical vein. The umbilical arteries carry deoxygenated blood from the whole body to the placenta which is the gaseous exchange site prenatally. On the other hand, the umbilical vein returns oxygenated blood from the placenta back to the fetus.
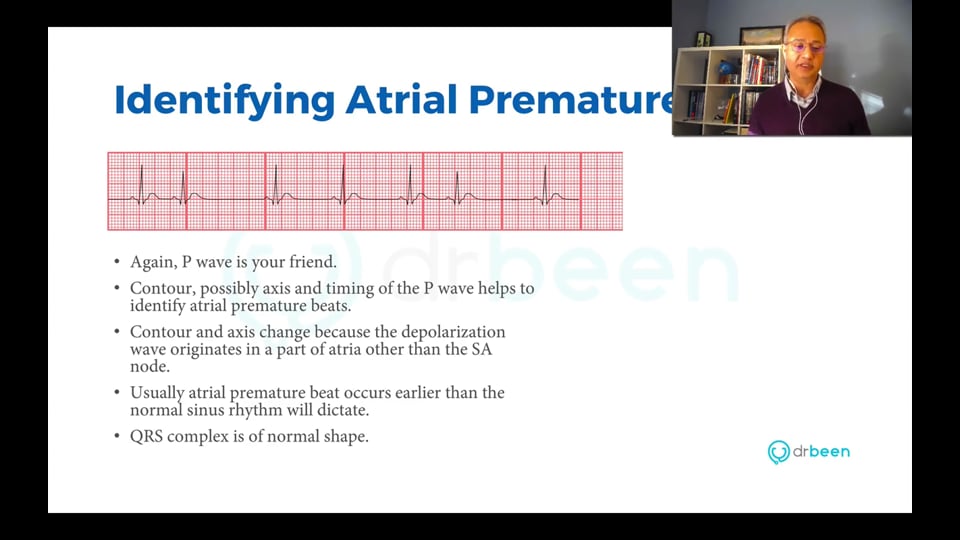
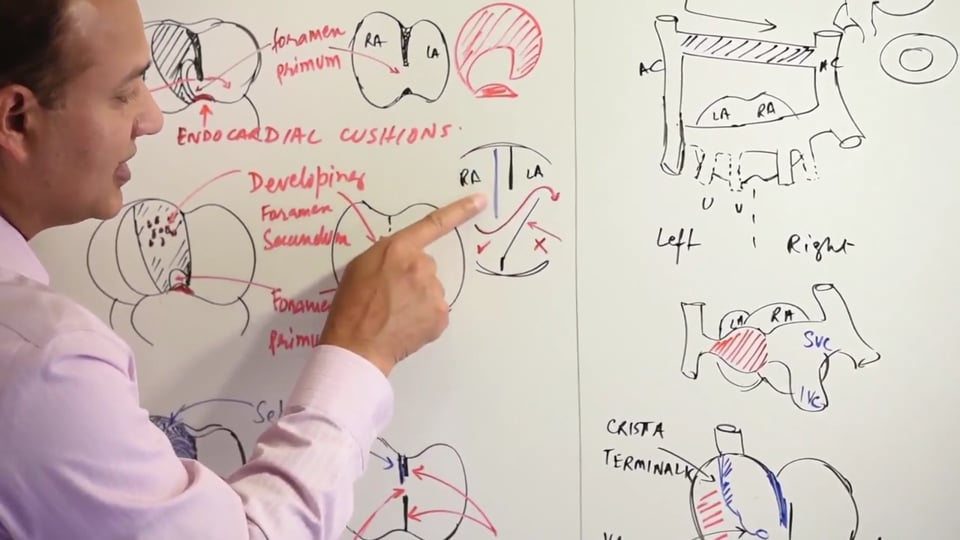
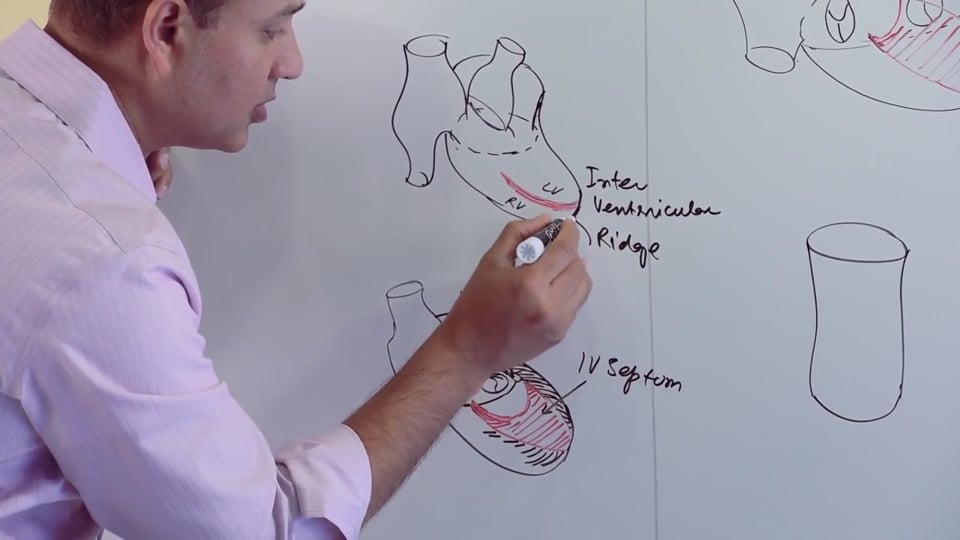
• The fetal heart has a right to left shunt in the form of a patent foramen ovale. This has extensively been discussed in the previous lectures. As part of interatrial septal development, the two septae (septum foramen and secundum) leave a defect in the interatrial septum which allows the shunting of the blood from the right to left atrium.
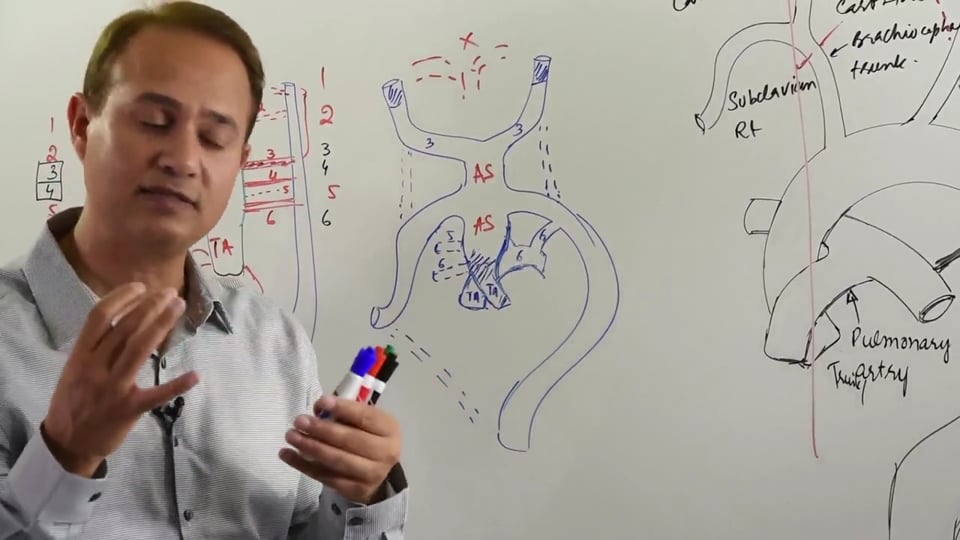
• The ductus arteriosus opens at the underside of the aorta and connects it with the pulmonary trunk. The role of ductus arteriosus and its situation just distal to the origin of the left subclavian artery will be discussed later into the notes.
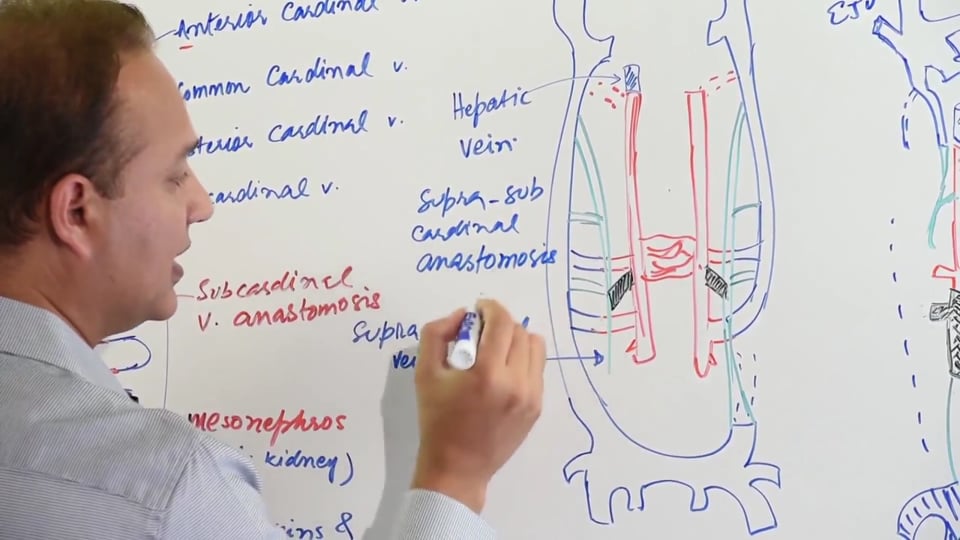
• Ductus venosus connects umbilical vein to the inferior vena cava, allowing the blood to bypass the hepatic route in doing so.
FLOW BEFORE BIRTH
Before birth, two umbilical arteries carry deoxygenated blood from the fetus to the placenta. Placenta allows gaseous exchange via diffusion to take place between the maternal oxygenated blood and the fetal deoxygenated blood. It's important to remember that the fetal and maternal bloods don't come into direct contact. Prenatally the fetal lungs are collapsed; hence placenta is the site of gaseous exchange before birth. Although the placenta has maternal deoxygenated blood but still it's able to provide fetus with its oxygen requirements. This is made possible by the higher oxygen affinity of the fetal hemoglobin, HbF. HbF has 2 alpha and two gamma globin chains, which allows it to extract oxygen from a relatively deoxygenated maternal blood.
Ductus venosus connects umbilical vein (coming from the placenta) to the inferior vena cava, thereby forming a shunt that allows half of the placental blood to bypass the hepatic route. Hence 50% of the oxygenated blood from the placenta enters the hepatic sinusoids. This blood that enters the hepatic sinusoids is returned via the hepatic veins to the inferior vena cava. All of the oxygenated blood doesn't enter the liver and the hepatic sinusoids because the passage through the hepatic sinusoids can take a very long time for the blood to reach the heart. The oxygenated blood in the IVC (80% oxygen saturation) at this point mixes with the deoxygenated blood from the hepatic veins (26% oxygen saturation). Before entering into the right atrium, the blood in the IVC has an oxygen saturation of around 67%.
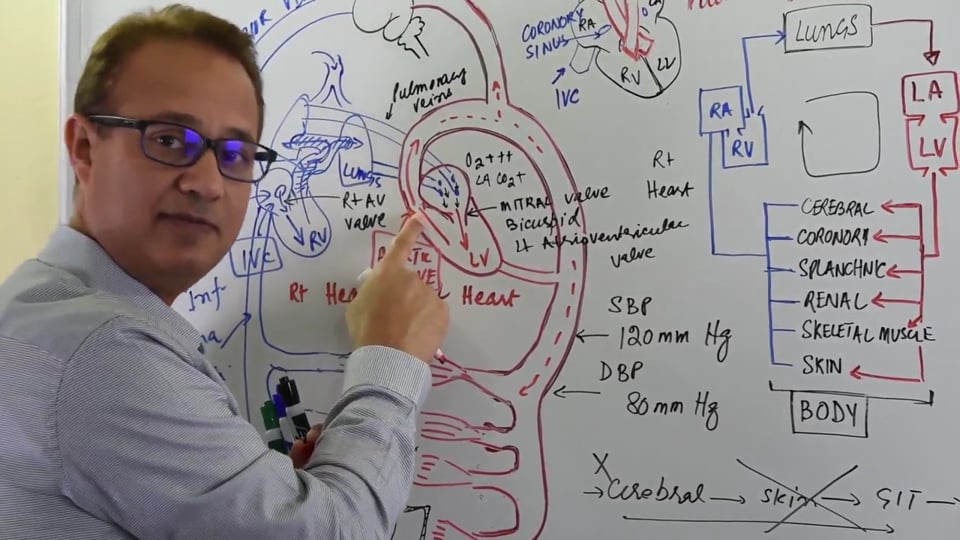
A hallmark of fetal circulation is that, the superior vena cava returns deoxygenated blood from the head, neck and upper extremities region to the right atrium. This deoxygenated blood reaching the heart via the SVC is directed into the right ventricle and subsequently into the pulmonary trunk. The inferior vena cava on the other hand brings relatively oxygenated blood (67% Oxygen saturation) to the right atrium, which due to flow dynamics passes through the patent foramen ovale into the left atrium. As discussed in earlier lectures, foramen ovale forms a right to left shunt which allows the oxygenated blood coming from placenta to bypass the pulmonary circuit. After birth, foramen ovale becomes obliterated and forms the fossa ovalis. Once it's in the left atrium, this relatively oxygenated blood (coming from right atrium via foramen ovale) goes into the left ventricles and subsequently leaves the heart via the aorta. Most of this blood then leaves via the three large branches of aorta (brachiocephalic trunk, left common carotid and the left subclavian arteries) towards the head, neck and upper extremities region. There's no mixing of the blood coming from SVC and IVC, though they're both received by the right atrium.
The deoxygenated blood (25% oxygen saturation) coming from the SVC entering the right atrium, is directed into the right ventricle and subsequently into the pulmonary trunk. The ductus arteriosus opens into the underside of the aorta, and connects the pulmonary trunk to the arch of aorta. Thus, ductus arteriosus forms a right to left shunt allowing the deoxygenated blood to bypass the pulmonary circuit. This shunting across the pulmonary circuit occurs because fetal pulmonary vascular resistance is very high resulting in just 10% of the right ventricular output goes to the lungs. The rest 90% of right ventricular output is shunted from the pulmonary trunk to the aorta. This deoxygenated blood from the SVC which is in the aorta, now mixes with the relatively more oxygenated blood which came from the placenta and passed through the foramen ovale.
As mentioned earlier, only 10% of the fetal right ventricular output is directed to the lungs. This blood is brought back to the left atrium by the pulmonary veins and it leaves the left side of the heart via the aorta. The blood in the aorta after the opening of ductus arteriosus is at an oxygen saturation of 60%. This blood via the descending aorta is now directed to the abdomen and lower parts of the fetus and finally reaches the internal iliac arteries. Most of the deoxygenated blood now enters the two umbilical arteries and is taken to the placenta. The umbilical arteries on their route to the placenta touch bladder as well. Later on, the proximal parts of the umbilical arteries later form the superior vesical arteries.
Levels of oxygen saturation in different fetal vessels in decreasing order of oxygen saturation:
• Umbilical Vein
• Ductus Venosus
• IVC
• Right Atrium
PRENATAL SHUNTS
Before birth there are 3 vascular shunts which allow bypass of the blood flow mainly around the lungs and the liver. These 3 shunts are right to left in direction and tend to close immediately after birth. These shunts are as following:
|
SHUNT |
ORGAN BYPASSED
|
|
Ductus Arteriosus |
Lungs |
|
Foramen Ovale |
Lungs |
|
Ductus Venosus |
Liver |
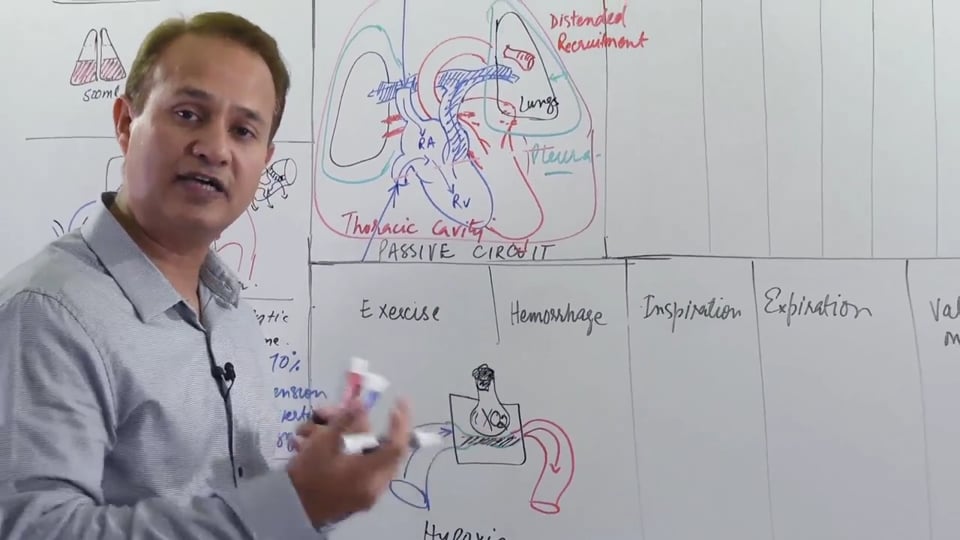
Earlier there was a brief mention of the high pulmonary vascular resistance and need for a shunt across the pulmonary circuit. Let’s touch that subject now in order to gain more clarity on this concept. Before birth the fetal lungs are collapsed. Since the fetus is inside the womb surrounded by amniotic fluid, the lungs are also filled with fluid and this keeps them collapsed. Since the lungs are collapsed as a result the pulmonary arterioles are also collapsed. This is because, the alveoli are filled with fluid at this point and the surrounding arterioles tend to exhibit vasoconstriction due to this resultant hypoxia (due to absence of oxygen in the alveoli). This hypoxic pulmonary arteriolar vasoconstriction results in a very high pulmonary vascular resistance and as a consequence the lungs remain in a collapsed state before birth. Since the right ventricle has to pump against a very high pulmonary vascular resistance, it results in the right ventricle being more hypertrophied than the left ventricle before birth. Fortunately only 10% of the right ventricular output flows to the lungs (other 90% is shunted across the pulmonary circulation by DA in the aorta) so the degree of hypertrophy isn't that pronounced at the time of birth. This situation is reversed within one month after the birth.
FLOW AFTER BIRTH, REASON FOR FLOW CHANGES & THE CHEMICAL SUBSTANCES INVOLVED
After birth, the 3 above mentioned shunts tend to close because of changes in pressure gradients and in oxygen tension. Immediately after birth, as the newborn breathes the lungs become expanded. As the alveoli expand, the pulmonary vasculature also tends to expands due to decreased effects of hypoxic pulmonary vascular resistance. This results in an overall decrease in pulmonary vascular resistance and blood from the right ventricle is directed via the pulmonary trunk towards the pulmonary circulation. The increased pulmonary blood flow to the lungs also results in an increased pulmonary venous return to the left atrium. Consequently left ventricular output increases and the aorta receives more blood resulting in an increase in aortic blood pressure. Hence, the increased pressure in the aorta tends to reverse the shunt across the ductus arteriosus. Overall the pressure on the left side of the heart tends to increase more than the right side of the heart. As the lungs become functional, the following changes occur:
• Increased bradykinin levels
• Increased oxygen tension (more than 50mm of Hg)
• Decreased PGE2 and prostacyclin levels
Overall, there's an increased oxygen tension due to expansion of lungs and an increased released of bradykinin from the lungs. Following this, there's an immediate drop in PGE2 and prostacyclin levels which were being produced as a result of hypoxia. Prostaglandin E actually is an inhibitor of contracting response of ductus arteriosus to an increased oxygen tension. An oxygen tension above 50 mm of Hg promotes the closure of the ductus arteriosus. Therefore, all the above mentioned changes result in the contraction of specialized smooth muscle in the walls of ductus venosus and ductus arteriosus. Consequently, DV and DA become obliterated over the next couple of hours after birth. Failure of the ductus arteriosus results in a patent ductus arteriosus after birth. The closure of ductus arteriosus is a slow event and it's summarized below:
|
Within few hours |
DA starts constricting |
|
Within 24 hours |
Obliterated in 40% of newborns |
|
Within 48 hours |
Obliterated in 80% of newborns
|
|
Within 96 hours |
Obliterated in 100% of newborns |
The umbilical vein also closes upon birth as the umbilicus is clipped and the connection between the placenta and the fetus is severed. Closure of umbilical vein reduces the amount of blood flowing via the inferior vena cava into the right atrium. Hence the right atrial pressure tends to further drop relative to left atrial pressure. The increased left atrial pressure results in fusion of the septum primum and secundum and the foramen ovale is subsequently closed. Closed foramen ovale is referred to as fossa ovalis. The floor of the fossa ovalis is formed by the septum primum and its margin called the limbus ovalis is derived from the septum secundum. Closure of the foramen ovale means that the right heart is connected to the pulmonary circulation and the left heart is connected to the systemic circulation.
Once the umbilical connection to the placenta is severed after birth, the ductus venosus also begins to start closing. The closure of ductus vensosus is a slow process and it can take a month after birth to completely become obliterated. In cases where the newborn is anemic, the ductus venosus can be cannulated from the outside to initiate a blood replacement therapy. Adult remnant of the ductus venosus is referred to as the ligamentum venosum.
REMANANTS IN ADULTS FROM THE FETAL CIRCULATORY SYSTEM
Postnatal changes which occur after birth result in formation of some adult remnants from the fetal circulatory system. These remnants and the changes after birth which give rise to them are summarized in the table below:
|
ADULT REMANANT |
CHANGES AFTER BIRTH |
|
1, Fossa Ovalis |
Closure of the foramen ovale
|
|
2, Ligamentum Arteriosum |
Closure of ductus arteriosus |
|
3, Ligamentum Venosum |
Closure of ductus venosus |
|
4, Medial Umbilical ligaments |
Obliteration of the distal part of the two umbilical arteries, proximal part forms superior vesical artery |
|
5, Ligamentum Teres hepatis/ Round ligament of liver |
Obliteration of the umbilical vein |
PATENT DUCTUS ARTERIOUS, ITS SIGNIFICANCE IN FETAL LIFE AND CLOSURE AFTER BIRTH
The ductus arteriosus is formed from the 6th pharyngeal arch artery on the left side. It connects aorta to the pulmonary trunk just distal to the origin of the left subclavian artery and forms a right to left shunt. This right to left shunt enables most of the right ventricular output to bypass the pulmonary circuit because the lungs are collapsed at this time and as a result the pulmonary vascular resistance is quite high. The ductus arteriosus is composed of specialized smooth muscle which releases PGE2 and prostacyclins in response to low oxygen tension/ relevant hypoxia. The PGE2 and prostacyclins release tends to keep the ductus arteriosus open before birth. Normally, the ductus arteriosus closes within few hours after birth due to contraction of the smooth muscle in its wall and is referred to as ligamentum arteriosum.
Congenital condition which can cause hypoxia after birth can prevent the ductus arteriosus from closing. One such condition is erythroblastosis fetalis. As mentioned earlier, the low oxygen tension due to hypoxia can cause a release of prostaglandins and prostacyclins which will prevent the ductus arteriosus from closing. Other than that, babies born with a preductal coarctation of aorta tend to have a patent ductus arteriosus which should be kept open. In case of preductal coarctation, the ductus arteriosus remains patent and provides blood flow into the descending aorta and thereby the abdomen and lower parts of the body. In situations where a left to right shunt is important for the survival of the newborn, the ductus arteriosus is necessary to be kept patent. Congenital heart defects such as transposition of great vessels requires such an intervention to keep the ductus arteriosus open. Prostaglandin E analogues such as dinoprostone, are administered in such cases which helps in keeping the ductus arteriosus patent.
In preterm babies, the lungs aren't fully developed, therefore after birth there is a decreased arterial oxygen tension and an increased prostaglandin E2 and prostacyclins synthesis in response to this relative hypoxia. Hence, the incidence of a patent ductus arteriosus is very high in preterm/premature infants. Patent ductus arteriosus results in a left to right shunt after birth, which is non-cyanotic and the newborn has a machine-like murmur audible upon auscultation. In such cases, prostaglandin E inhibitors such as indomethacin and ibuprofen are administered in order to promote the closure of ductus arteriosus.
Foramen ovale: to keep the foramen ovale open in TGA atrial septoplasty is done.
The situation of ductus arteriosus just distal to the origin of left subclavian artery has great significance. Most of the oxygenated blood entering the right atrium is directed towards the head and neck region via the 3 branches large branches of the arch of aorta. Just distal to the origin of subclavian artery, the aorta is connected to the pulmonary trunk via the ductus arteriosus. At this point the deoxygenated blood (coming originally from the SVC) in the pulmonary trunk is shunted into the aorta (via DA) and is allowed to mix with the oxygenated blood which originally came from the placenta. Hence, most of the oxygenated blood from the placenta directed to the head and neck region which at that that point of development has greater oxygen demands. This remaining blood in the aorta, after it has mixed with the shunted deoxygenated blood from the pulmonary trunk, has an oxygen saturation of 50% and is now directed to the rest of the body (abdomen and lower limb).
In this video we will learn about :
1. Fetal circulation pathway.
2. Shunting of blood in fetus.
3. Chemical substances starting the flow.
4. Flow dynamics.
5. Changes at birth.
6. Remnants of fetal circulation components.
No credit card information needed.












Write A New Comment
1 Comments
d.caine@*.com
Sep 12 2020, 9:30 am
Excellent thank you! I have read about the 'blood volume' theory of adaptation to extra uterine life. In this theory it is the increased blood supply to the lungs that makes arterioles turgid. The arterioles sucaffolding the alveoli have the effect of opening the alveoli. What is your opinion about that theory? Thank you